

The Perspectives and the Biopsychosocial Model
At first glance, the perspectives methodology may seem to be Adolf Meyer’s psychobiology revisited. As later developed by George Engel, the biopsychosocial model urges clinicians, in treating their patients, to take into account aspects of biology, psychology, and culture. In recent years, the model has been of special interest in the treatment of psychosomatic conditions such as chronic pain, where it has proved effective. In psychiatry there has been a renewed call for research on the integration of pharmacotherapy and psychotherapy in the name of biopsychosocial integration.
What, then, is the relationship of the perspectives model to the biopsychosocial model? Simply put, the perspectives provide a method of using the central insight of the biopsychosocial model: that there are multiple determinants of behaviors and conditions arising from biology, psychology, and the social and physical environment. Because nothing a priori is excluded in the biopsychosocial model, its application can pose a heuristic challenge. Recall that Engel’s levels of organization in his systems hierarchy spanned everything from subatomic particles to the biosphere. Granted, no clinician or researcher attempts to consider and control for the universe of possible factors; nevertheless, methodological assistance is needed to decide how to go about considering the literally “too numerous to number” factors that make up our biopsychosocial world – canadian health and care mall.
Enter the perspectives methodology. The perspectives take on the challenge of the biopsychosocial approach to consider nearly everything in the formulation of the individual case and to organize the data into four major perspectives. Employed diligently, these organizing perspectives assist the clinician to consider, if not “everything” in the biopsychosocial universe, at least a great deal more than he or she might consider without the methodology. In addition, the repeated interaction of the perspectives assists the clinician to link together the various strata of the biopsychosocial model in an effective treatment approach.
In the most recent description of his perspectives, Paul McHugh places “the perspectives into a view of human mental life as organized hierarchically into four distinct but interrelated domains from the most neurologically basic to the most individually highly developed.” Table is McHugh’s scheme of how the perspectives relate to each other in the biopsychosocial world and, even more, how they address modes of mental disorders and basic treatment goals. Each of these components interacts with the others; the table expresses how the perspectives are structured from the most basic neurological level to the most complex cognitive one.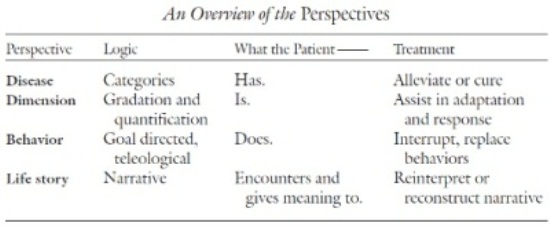
Clearly, then, the perspectives methodology is not antithetical to the biopsychosocial model. In addition to the organizing function, at least three of the four perspectives—disease, behavior, and life story perspectives— assume there are biological and psychosocial components in the genesis and treatment of psychiatric disorders. The remaining perspective, dimension, seeks to measure constructs that are biological, cultural, and psychological. In that sense, the perspectives are built on and employ the biopsychosocial model.
The perspectives thus are a methodological supplement to the biopsychosocial model, because they help organize and apply the latter model in the individual cases presented to a mental health clinician. If the biopsychosocial model is a unified theory that seeks to explain all causes, the perspectives are much more modest in their aim. The perspectives model suggests the methods one might employ to put the biopsychosocial model into rational practice. In many ways, the perspectives are the operational testing and application of biopsychosocial theory.
The perspectives help one to avoid using a ritualized invocation of the biopsychosocial model and then proceeding with a treatment regimen that ignores key elements. A recent survey of 54 (of 118 polled) U.S. medical schools suggested that while many attempts are made to teach biopsychosocial medicine to future physicians, there are generally still barriers in the development of a unified curriculum that might be described as “biopsychosocial.” This survey of medical schools is prob ably a good indication of most treatment approaches today: the biopsychosocial is invoked as the model guiding evaluation and treatment, but barriers remain to its being as influential as it might be. The perspectives are an attempt to provide a way of increasing the effectiveness of the biopsychosocial model.
Just as with the biopsychosocial model, it is not a question of “new” knowledge in employing the perspectives. Every aspect of the perspectives has already been written about and employed clinically. It would be erroneous, therefore, to expect some new information from the perspectives themselves. What is original is the structured organization of the perspectives. The essence of the working of the perspectives is dialectical. They take the clinician’s “I know such and such” and invite him or her to hear, “But you must also consider your patient from this other perspective.” Then, from the application of the newly adopted perspectives, the clinician achieves a fuller appreciation of the disorder and approaches for treating the disorder.
